Below is a letter I recently sent to Ontario’s Minister of Health and Long-Term Care, Christine Elliott. The letter was written following a number of very disappointing decisions I received from the College of Chiropractors (CCO) of Ontario concerning a number of complaints I have submitted over the past couple of years (details to follow soon).
The CCO has made it clear that they are either unable or unwilling to hold chiropractors to a reasonable ethical or scientific standard for the protection of the public. I have submit complaints detailing how Ontario chiropractors have used deceptive advertising, how they have disseminated provably false claims, how they have misled the public on scientific and medical issues, how they have cautioned that vaccinations are “toxins”, how they have lectured that medical doctors “kill” their patients, how they have endangered lives by claiming such nonsense as one cannot overdose on vitamin D, how they have made false claims supporting invalid tools and techniques, how they have exposed patients to x-rays unnecessarily, how they have targeted patients with predatory sales tactics, and how they have shown a blatant disregard to their responsibilities as regulated health professionals. No single chiropractor has been disciplined for any of the above issues.
I am at wit’s end. The regulatory college is not effective and not appropriately acting on its mandate to protect the public. I have been reasonable and gone through the proper channels by submitting complaints, but now I realize that chiropractors are not capable of self-regulation. There are many great chiropractors who initially gave me hope that the profession could reform itself, but I no longer see this as a realistic possibility. The profession must either be dismantled or there must be intervention by independent authorities.
We are increasingly aware of the danger that health and science misinformation both pose to public health, democratic decision making, and the public’s understanding of science. The chiropractic profession was given a chance to regulate themselves and improve. They have collectively failed.
The Letter
Dear Minister Elliott,
Several years ago, while completing my PhD, a colleague of mine handed me a pamphlet advertising an event put on by a local chiropractor. Curiously, the topic of the seminar was cancer, but chiropractors are not medical doctors and certainly not specialists in oncology.
As I learned more about this practice, I found that the chiropractic profession harbored strange beliefs surrounding medicine generally. While some practice akin to physical therapists, there exists a large subset of practitioners who believe that spinal “adjustments” are the core requirement to maintain good health and prevent disease – a provably absurd notion. The philosophy behind this belief is even more absurd, but I will spare you the details.
At the time, I was most passionate about science education, but I felt that my efforts were undone by regulated practitioners who disseminated misinformation to large audiences, utilizing their authority as health professionals to deceive the public for financial gain. This was the beginning of my adventure in science advocacy in activism.
Learning of the existing regulatory mechanisms in place that are intended to protect the public, I began systematically submitting complaints against practitioners to The College of Chiropractors of Ontario. Most recently (today), I submitted a complaint concerning two chiropractors who claim that vaccinations are the “absolute number 1 chemical stressor” requiring chiropractic treatment. This is merely a sampling of the many absurd and dangerous claims I encounter daily.
Unfortunately, the regulatory college has failed to appropriately act on complaints. Recent stories in various national outlets (some of which have featured my activism) highlight the extent of the issue and shed light on a greater regulatory failure: The College of Chiropractors of Ontario itself is comprised of council members who harbor pseudoscientific beliefs, including a strong opposition to immunization. In the midst of low vaccination rates and increasing outbreaks, this is completely unacceptable.
I have – thus far – played by the regulatory rules and mechanisms available, but they are simply inadequate. For the safety and general good of the public, I ask that you intervene with the College, review complaints, and enact stronger regulation. As with other health professionals, chiropractors operate within a privileged marketplace. It is time that the profession took on the responsibility that comes with that privilege.
Success in the vast marketplace of natural health products is no easy feat. Where does one begin? Well, you could find a unique ingredient in the wild with some as of yet unknown medicinal properties. However, you would need to identify the valuable ingredient, demonstrate a potential medical use, ensure safety in effective doses, run clinical trials, register with Health Canada, and finally figure out bulk production. I’ll be honest with you, I’m not about to go to the trouble.
So why not take a few shortcuts? Why not identify an existing ingredient that already has Health Canada approval and then simply re-appropriate the ingredient for a similar, but distinct medicinal use? Give it fancy branding and position it as a unique product within the marketplace, permitting significant mark up. Without the serious science, the product will need something to lend legitimacy; maybe association with a major research institution or university? Bingo.
Entirely unrelated to the above hypothetical, I recently came across an article by Global News published earlier this month promoting a new “Hangover Pill” created in Manitoba. I immediately rejoiced; as documented by the World Health Organization, hangovers are the leading cause of death in the developed world and the second leading cause of getting up late on Sundays. What’s worse, there is no known preventative measure; it could happen to anyone at any moment. Just kidding, that’s bullshit. So, too, is the article.
The article describes a hangover remedy called Clear Head. If you’ve been drinking and that’s too difficult a name to remember, don’t worry; the article names the product a whopping 7 times. Read on and you will get it eventually. What you won’t get is any serious science or skepticism.
The article claims that “Clear Head works to counteract the action of [brain receptors]” and also “helps the liver clear the toxins.” Ah, of course! It’s those pesky toxins again. The product’s origin story is even more dubious.
Alex began researching vitamins and ingredients he thought might help with his dreaded hangovers.
“I compiled a list of products I thought would help me,” he said. “I started to divide and conquer these ingredients by experimenting on myself and friends to better understand what is the actual ‘magic’ ingredient.”
Well, that sounds both scientific and ethical. Luckily, Alex realized that experiments on his buddies might not be the most valuable in developing a health product, so he passed the torch to his father Ron Marquardt – a professor at the University of Manitoba. The team also enlisted the help of marketing specialist and distributor Ray Takacs, who is careful to only make reasonable scientific claims when promoting the product.
Oh, never mind. Well with that confidence, there must be some high-quality evidence supporting this product. Let’s start with what we know from the original promoter – ah hem – I mean reporter. What evidence is reported?
“Clear Head was developed at the University of Manitoba and has a Health Canada stamp of approval.”
None, of course, but why bother with science when we can invoke scientific authorities? But wait; are these legitimate scientific authorities?
Let’s start with Health Canada. As I’ve noted in the past, Health Canada – despite their claim otherwise – does not require a product to demonstrate efficacy prior to registration as a natural health product. In place of legitimate evidence, Health Canada permits “traditional use claims,” meaning if someone has used some natural product in the past for anything and sufficiently documented it, the text – scientific or not – can be used in place of sound evidence (with minor restrictions). If anyone from Health Canada is reading, I want you to know that you are doing a bad job and should feel bad.
I’m sure you know where this is going: Clear Head’s registration with Health Canada relies not on well-designed clinical research, but on traditional use claims referencing monographs that existed long before the product. Although the main ingredient – silybum marianum (milk thistle extract) – has been examined as a potential “liver protectant,” it has failed to pass the rigor demanded of clinical trials.
A 2007 Cochrane review noted that there is no reliable evidence supporting its use. Higher quality evidence tended towards negative results, which is expected in the absence of a real effect. A 2012 randomized controlled trial (RCT) did not show any liver benefits for subjects with hepatitis C. Oh, and a 2017 systematic review of biochemical indicators of silymarin effects in patients with liver disease concluded results were “without clinical relevance.” Worse still, not a single RCT has been published on silybum for hangovers. Even Health Canada’s monograph does not mention hangovers once. Oops!
Maybe it will evolve into a morning Caeser or something?
Perhaps the reporter should have looked this information up before publishing a suggested dose:
Each packet comes with four capsules. People take two before consuming alcohol and then one more before they go to bed. The fourth is a spare, to take the next morning if you need it.
Then again, can we blame her when a CBC reporter failed the same critical thinking step before reporting nearly identically two years earlier (2016):
Each packet comes with four capsules and you’ll need to take two before consuming alcohol and then one more at the end of the evening. The fourth is a spare, in case you need it the next morning.
A simple perusal of the product’s website should be enough to sense that straws are being grasped at to legitimize the product; the site offers a single testimonial and a “Why It Works” page that provides no evidence supporting the claim that this hangover cure “actually works.” Can you spot the appeals to nature and tradition?
All natural ingredients
Clear Head is prepared from an extract of Silybummarianum [sic] (Milk Thistle). The active compound in the extract is silymarin. This extract has been used for over 2000 years to treat a range of liver diseases. More recently, it has been shown to be effective in the relief of symptoms of hangovers.
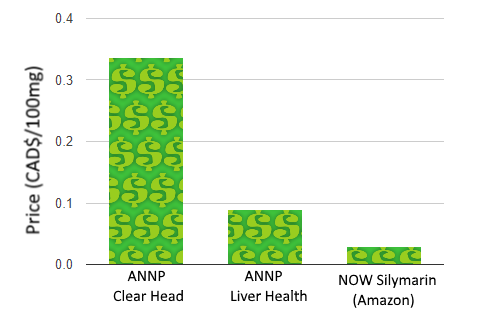
A look at the ANNP’s website also reveals that the ingredient is not novel. While you can pick up 12 pills of ANNP’s Clear Head for $10, they also offer a silybum product without the Clear Head branding at $21.16 for 90 pills. If you’re not convinced the products are identical, Health Canada includes both under the same registration initially licensed in 2010.
Oh, you sneaky marketing folk.
Wait a minute . . .
Of course, you can also find silymarin much cheaper on Amazon, but perhaps lacking the backing of a research institution.
To be fair, bulk pricing does come into play, and ingredient sourcing and concentrations may differ slightly, but there is no strong evidence either way to support one product over any others.
If we were to base our purchase on the product making the most grandiose and unsubstantiated health claims, however, ANNP’s Liver Health steals the show:
This slideshow requires JavaScript.
While none of these claims are supported by high-quality evidence, there is something more troubling here: these are unambiguous schedule A disease prevention claims in the context of product marketing. While Health Canada permits direct-to-consumer prevention claims for natural health products, the claims must first be authorized. As none of these claims are supported by the product’s registration, why exactly would Health Canada permit them?
When it comes to the product’s relationship with the University of Manitoba (UM), the story gets more complicated. You would think the connection is straight forward considering Clear Head’s Facebook page proclaims that Clear Head was “Created at the University of Manitoba!” ANNP has even deemed the relationship important enough to place on marketing material.
I’m sure this isn’t an important feature of their marketing campaign. Source.
What’s up with that? Well, UM is home to the Richardson Centre for Functional Foods and Nutraceuticals (RCFFN) – a “bioprocessing and product development facility” whose mission is to “lead functional food and nutraceutical research for the improvement of health and nutrition” and “support the development of an economically viable functional food industry.” The RCFFN hosts the aforementioned ANNP, who developed the Clear Head product. Just as in their ad, the Clear Head website prominently brandishes this connection:
Developed at the Richardson Centre for Functional Foods and Nutraceuticals at the University of Manitoba.
Yet the RCFFN merely leases space and equipment, prominently indicating on their website that ANNP is a tenant. To say the product is developed at the University of Manitoba is true geographically, but the product is not developed or endorsed by the University of Manitoba. In fact, there is no indication that any clinical research on the product has been performed at the university. It is, however, developed by professors at the university.
Heading up the ANNP is the aforementioned professor, Ronald Marquardt – ANNP president, UM professor, and Clear Head “developer.” Dr. Peter Jones – a scientific and business adviser with ANNP – is the Director of the RCFFN at UM. I was unable to find publications by either professor on hangovers or silymarin. I reached out to the RCFFN, ANNP, and the professors. Vice President and R&D Director of ANNP, Dr. Suzhen Li, got back to me.
Regarding the evidence for Clear Head, Dr. Li directed me to Google Scholar, noting that there is “a very large number of scientific publications on silymarin dealing with the safety, efficacy, mode of action, etc.” She went on to list the number of publications containing relevant keywords in the title: “milk thistle” (944) and “silymarin” (2880). There are no publications that include both “silymarin” and “hangover” in the title, but Dr. Li noted that 568 publications contain both keywords in the text.
The large number of results indicates that there has been interest in the area, but it has no bearing on whether these compounds are valuable for anything. For example, the same search for “homeopathy” returns 5,280 results, yet we know that homeopathy is an implausible concept. In addition to quantity, we must consider the precise question that each study addresses and how rigorously the question is addressed.
In addition to highlighting the quantity of results from various search queries, Dr. Li provided the results from some, claiming that they “demonstrate that silymarin has many different beneficial effects in humans and animals.” Still, none of the studies are clinical trials examining silymarin and hangovers. I address each study in the Appendix.
While milk thistle and silymarin do appear to possess some interesting properties and biochemical interactions, the failure of the literature is in making the transition from the basic sciences to the clinical sciences. The distinction is quite important, but too often ignored in the pursuit of promising therapies. In essence, basic science involves research looking at the low-level mechanisms, often in a laboratory setting. For example, if we were looking for a novel compound to eradicate cancer cells, we might first test the compound in vitro on cells in a petri dish. Unfortunately, the success of such an experiment tells us very little about clinical applications.
Let’s suppose – for example – that we were examining bleach as a potential chemotherapy. While bleach would undoubtedly kill cancer cells in our petri dish, there remain unanswered questions required to make the leap to clinical applications. What is the toxicity of the compound and what are the side effects? How is it best administered? What is the optimal dose? What is the bioavailability? Does it make a meaningful clinical impact? Does it work generally at a population level or only under specific conditions?
In the case of bleach, we know that it does not satisfy these criteria as a cancer treatment. With novel compounds, there is an additional risk: there is a good chance that our knowledge of the basic science is incomplete. A popular example reader’s should be familiar with is the hype behind anti-oxidant supplementation. While our initial conceptualization of cellular metabolism demonized reactive oxygen species, contemporary research indicates that excessive anti-oxidant supplementation is not necessarily a good thing. As with most biological processes, the human body is often capable of maintaining a balance from a healthy diet alone.
For these reasons, I find the confidence of marketing claims for silymarin troubling. As in the Global News article, Dr. Li noted that “milk thistle’s ability to mitigate hangover was discovered by Alex Marquardt” and has been “confirmed by positive feedback response from many different users and by researchers,” yet this is not actual confirmation from RCTs.
First the apple, now this?
If you are not yet scientifically triggered, look at how ANNP represents Health Canada licensing on their website:
In Canada all nutraceutical products must be licensed and issued a Natural Product Number (NPN). Products that are licensed have been shown to be safe (minimum of two clinical trials with humans) and effective (minimum of two clinical trials). Some companies market nutraceutical products that are not approved by Health Canada and often do not have the recommended concentration of active compound. Products that do not have a Health Canada NPN should not be purchased.
Based on this claim, would you not expect that products you buy from ANNP have been validated by two clinical trials demonstrating efficacy? At very least, should there not be a single, high-quality, double-blinded, and randomized study showing that individuals taking silymarin reported less severe hangover symptoms compared to those taking a placebo? Dr. Li responded to my concerns regarding their representation of Health Canada licensing:
This is a stated requirement by Health Canada and repeated by ANNP. Please consult the Health Canada milk thistle monograph to see if this is correct and, if not, please contact Health Canada to determine why they have issued an NPN for milk thistle to many companies containing 80% silymarin. We believe that some traditional medicine such as milk thistle can be issued NPN’s without safety and efficacy trials if they have been successfully used as a traditional medicine. You need to discuss this with Health Canada.
Dr. Suzhen Li, ANNP Vice President
Indeed, Health Canada’s registration notes traditional use claims. Again, this is a failure of Health Canada to properly require evidence of efficacy, but that’s no excuse to represent the product as proven effective. Regarding ANNP’s claims marketing their Liver Health product (such as “Cancer Prevention“), these claims were authorized by Nelson Pereira of Health Canada’s Inspectorate Program. I reached out to Health Canada and Nelson Pereira for comment, but have not yet heard back. I’m very interested to hear about the evidence Health Canada relies on to authorize these claims. After all, if milk thistle really could prevent cancer, wouldn’t we all want to be taking it?
In addition to the citations provided in the Appendix, Dr. Li provided me with a brief document outlining the basic research behind hangovers and the potential role of silymarin. While some of the research was interesting, there was still no clinical research in humans examining the benefits of silymarin for clinical endpoints related to hangovers.
Despite the lack of evidence demonstrating the product to be effective, ANNP has pushed forward, partnering with distributor T.H.E Food Source, and marketing the product to credulous reporters, radio shows, and “natural health” stores. They have even begun looking for Chinese distributors.
In all this marketing madness and curative certainty, only one limitation of Clear Head is offered:
If you go out and challenge it . . . you’re going to hurt.
So just don’t drink too much or it won’t work. This isn’t the first “hangover cure” that isn’t supported by clinical evidence and I doubt it will be the last. Bad journalism, bad marketing, bad regulation, and bad science are the status quo. As always, don’t buy the hype.
——————————————————————————————————————————————-
Acknowledgments
Thanks to Dr. Terry Polevoy for bringing this issue to my attention.
——————————————————————————————————————————————-
Appendix: Selection of Milk Thistle and Silymarin Studies
The following studies were sent to me by ANNP. I provide a brief summary below each. None of them examined clinical efficacy of silymarin for hangovers. Overall, my impression was that the totality of the evidence simply does not support the hypothesis that milk thistle supplementation provides any meaningful benefits. A number of sources note that oral supplementation results in poor bioavailability. Additionally, although milk thistle is well tolerated at typical doses, side effects do occur, often in the form of gastrointestinal distress. Allergies may also be somewhat common.
Perhaps most telling is that US-based NCCIH (National Center for Complementary and Integrative Health) – the NIH’s most infamous center – admits that “we know little about whether milk thistle is effective in people, as only a few well-designed clinical studies have been conducted.”
(Note: papers that appeared in multiple search results were only included in the first seen query section).
This was published in a low-quality journal “Integrative Cancer Therapies” and even they concluded: “The future of milk thistle research is promising, and high-quality randomized clinical trials on milk thistle versus placebo may be needed to further demonstrate the safety and efficacy of this herb.“
Another low-quality journal “Alternative and Complementary Therapies,” this is simply a narrative review written by an herbalist and naturopath. In their conclusion they reveal both their scientific ignorance and the lack of evidence: “Second, given the safety profile of the herb, clinicians would be well-advised to expand their use of this plant although clinical studies are lacking.” Just because something is relatively safe, does not mean it should be used clinically. Then again, that’s an apt summary of the naturopathic profession.
This paper simply noted that products prepared with milk thistle could include significant amounts of copper, which should be avoided by patients with Wilson’s disease.
This review noted that the flavonoids in milk thistle (the compounds generally considered to be ‘active’) have poor bioavailability. Instead, they examined a related compound and noted that it “provides significant liver protection and enhanced bioavailability over conventional silymarin.” This doesn’t exactly make a great case for Clear Head . . .
This review concluded: “We found no reduction in mortality, in improvements in histology at liver biopsy, or in biochemical markers of liver function among patients with chronic liver disease.” They noted the data were too limited to “support recommending this herbal compound for the treatment of liver disease.“
This Cochrane review concluded: “Our results question the beneficial effects of milk thistle for patients with alcoholic and/or hepatitis B or C virus liver diseases and highlight the lack of high-quality evidence to support this intervention.”
This was a review for veterinary applications in a veterinary journal that concluded: “Future study is justified to evaluate dose, kinetics, and treatment effects in domestic animals.”
This review’s conclusion is similar to my own conclusions: “while Silybum marianum and its derivatives appear to be safe and the available evidence on the mechanisms of action appears promising, there are currently insufficient data from well-conducted clinical trials to recommend their use in patients with alcoholic liver disease.”
This is another narrative review published in a low-quality journal. Even so, it concludes: “available evidence is not sufficient to suggest whether milk thistle may be more effective for some liver diseases than others or if effectiveness might be related to duration of therapy or chonicity and severity of liver disease.” In other words, there is no high-quality evidence on the topic.
This study examined in vivo effects of milk thistle supplementation and found that – contrary to in vitro studies – it is not a potent modulator of CYP2D6 activity. On the one hand, this means that concomitant supplementation milk thistle with CYP2D6 substrate drugs is unlikely to result in interactions, but, on the other hand, this demonstrated the failure of milk thistle to impact a biochemical pathway that may have been expected from basic science research and animal studies.
This Cochrane review concluded that milk thistle “does not seem to significantly influence the course of patients with alcoholic and/or hepatitis B or C liver diseases.“
This review concluded: “clinical efficacy of milk thistle is not clearly established. Interpretation of the evidence is hampered by poor study methods and/or poor quality of reporting in publications.” In terms of side-effects, “available evidence does suggest that milk thistle is associated with few, and generally minor, adverse effects.”
Though the article is referenced as being published in the Indian Journal of Medical Research (a rather low-quality journal), this narrative review is hosted on the site RedOrbit, which appears to be news, but is merely a promotional outlet. This article is simply not even worth addressing.
Regarding the properties of silymarin, the study concludes: “studies evaluating relevant health outcomes associated with these properties are lacking.”
It’s nice to see an RCT, but the paper was published in a low quality journal and suffers from methodological issues. I won’t perform a full analysis as the paper concerns diabetes.
This is another low quality journal and review. How shoddy is this journal? Well when I opened the link there was a fucking animated skeleton telling me to participate in a survey to win a prize. Alternative medicine journals: always good for a laugh. The earlier referenced Cochrane review performed a review on the same subject only a year earlier and with greater rigor. Refer to it.
This was a low quality RCT examining silymarin supplementation among β‐thalassemia patients. The study isn’t relevant to this article, but for curious readers, I recommend taking a look at Tables II and III for some glaring issues in this study.
Another low quality journal, however, they do report some promising initial results for NAFLD markers, although clinical outcomes were not evaluated. Again, this is not a study on hangovers.
Low quality journal, some methodological issues, and concerning diabetes again. As an aside, the Editor in Chief of the journal (Phytomedicine) is the head of research & development at Swedish Herbal Institute, a company which essentially uses bad science to market dubious products. Sound familiar?
Why? Why does this exist? Regardless, the study is not relevant and I haven’t the time to describe every methodological issue. Refer to Table 3 to see where the authors went fishing for significance with dynamite.
Another masterpiece published in Phytomedicine. I’ll just leave this portion of the conclusion here: “our results suggest that standard recommended doses of silymarin are safe and may be potentially effective in improving symptoms of acute clinical hepatitis despite lack of a detectable effect on biomarkers of the underlying hepatocellular inflammatory process.” The authors also concluded that “patients receiving silymarin had earlier improvement in subjective and clinical markers of biliary excretion,” which can be decoded from science-speak to “we didn’t find the result we were looking for, so here’s an artefact of our poor methodology to help get this published.“
Conclusion: “There is no evidence that silymarin affects viral load or improves liver histology in hepatitis B or C. No studies were found that investigated the use of silymarin concomitantly with interferon, nucleoside analogues, or other conventional treatments for hepatitis B or C. In conclusion, silymarin compounds likely decrease serum transaminases in patients with chronic viral hepatitis, but do not appear to affect viral load or liver histology.”
Again: “the main drawback of silymarin is its poor solubility therefore different approaches are been taken to enhance the solubility in turn the bioavailability of the drug.”
“Whether the protective administration of silymarin could be an effective clinical pharmacological strategy to prevent DIN is a question that remains to be answered in clinical trials.“
This is a poorly done review that even fails in some areas of basic science, and relies heavily on studies in rats to draw conclusions. They conclude, as they should: “well-designed clinical studies are urgently needed to evaluate the full potential of these natural agents to effectively treat or reduce the risk for liver cancer.”
Perhaps the lowest quality journal yet. The ‘study’ is worth a read if you’re looking for an example of how to avoid thinking critically and how not to perform a literature review.
If you’re not familiar with former doctor Andrew Wakefield, here is a quick primer: Mr. Wakefield was (and continues to be) primarily responsible for the widespread misconception that there is a possible link between autism spectrum disorders and vaccination. In 1998, Wakefield published a case series of 12 children where he suggested a link between gastrointestinal disease, autism, and the measles, mumps, and rubella (MMR) vaccine. In addition to the study entirely lacking scientific merit and rigor, investigative journalist and pharmaceutical critic Brian Deer uncovered fraudulent reporting and serious conflicts of interest. Despite all appearances, Wakefield was not an objective researcher, but was funded by a legal team launching a class action lawsuit against MMR manufacturers. In addition, Wakefield had previously applied for a single-jab measles vaccine patent. Wakefield possessed not one, but two serious conflicts of interest where he stood to benefit financially by slanting his research.
The legacy of Wakefield’s misinformation campaign.
In addition to retraction of his original paper from The Lancet, the UK’s General Medical Council revoked his medical license and barred him from practicing medicine. Beyond the fraud and dishonesty, they found that Wakefield acted with “callous disregard for any distress or pain the children [in the study] might suffer.” Despite being one of the worst medical and scientific debacles in modern history, Wakefield used it to his advantage by becoming the ‘expert’ voice of the anti-vaccine movement, enriching himself while deceiving the public at large.
Today, Wakefield has started life anew in Texas where he producesanti-vax conspiracy documentaries and influences gullible celebrities and politicians ranging from Jenny McCarthy – who helped popularized the anti-vax movement in North America – to Donald Trump, who – despite not possessing basic critical reasoning skills – is the current president of the USA.
How could he be a stable genius if he was vaccinated?
But that’s not all Mr. Wakefield occupies his time with; he also is quite engaged in speaking tours and evidently takes any platform that will host (and presumably pay for) his propaganda. Of course, this has all been written about quite extensively. So what’s left?
What’s left is the big picture. What’s left is Andy Wakefield’s evolution from a medical doctor and researcher to full-time charlatan who profits from fear and paranoia. The progression of Wakefield’s career and scaremongering is worth examining because it illustrates how a lack of moral regard (a callous disregard, if you will) can be used to fuel a movement built on conspiracy and distrust of expertise.
These points are important to emphasize because of how Wakefield is viewed and idolized by his supporters; they see him as a public defender who has been demonized by a vast conspiracy. The foundations of this belief, however, rely on Wakefield’s integrity as a fervent pursuer of truth. Such a characterization of Wakefield couldn’t be further from reality.
Since the initial scare and fallout from Wakefield’s fraudulent paper, a substantial effort has been put into examining the safety of vaccinations and their ingredients, including multi-dose vaccines like the MMR that Wakefield initially raised concerns over. These studies have continued to affirm the safety of existing vaccination schedules and have dismissed links between autism and vaccination. An honest scientist would admit the failure of their pet hypothesis, but Wakefield’s approach has been profoundly different.
Wakefield was recently invited to give a speech on vaccination at the less-than-reputable chiropractic college Life University. Did he give a balanced and comprehensive talk on current state of immunization science? Of course not.
Andy delivered an hour of anti-vax propaganda going as far as claiming that measles might have offered benefits if it continued to infect us. He claimed that vaccination has “destroyed herd immunity.” He claimed that we will experience a “plague” of neurodevelopmental disorders and allergies in children as a result of vaccination. He claimed that vaccines will increasingly fail at protecting us from the contagious diseases they prevent. He even suggested that vaccination may cause the next great extinction.
Crazy ol’ Andy “vaccines are causing a mass extinction of humans” Wakefield
It’s important to note how this speech should continue to undermine what little credibility Wakefield has left. In addition to diverging from scientific and medical evidence, Wakefield has evidently changed his stance from “vaccine safety advocate” to “vaccines are bringing the apocalypse.” This is important because Wakefield’s proponents often portray him as someone who is supportive of vaccination generally, but critical of vaccination schedules. This is obviously no longer the case.
Watching his speech, it’s clear where Wakefield’s talents lie; he is a persuasive and captivating speaker who knows precisely how to engage his target audience.
😂😂😂😂 Oh, please.
Ironically, the only impending apocalypse from infectious diseases will be a result of anti-vax efforts as measles outbreaks once again plague developed nations and polio reemerges in areas of low vaccination. Wakefield’s advocates need to recognize that his approach has evolved in exactly the way one would expect to capitalize on the anti-vaccine movement. His game isn’t science; it’s fear.
No more than a year ago, my preconception of chiropractic was probably similar to that of most Canadians; I assumed that chiropractors were doctors who specialized in back pain as it relates to the spine and musculoskeletal system. As I began to research chiropractic – dissecting both modern practice and historical origins – I found that this simplistic understanding did not account for the wide variety of diagnostic and treatment paradigms that practitioners adhere to. While many chiropractors are experts in the domains of pain and function in relation to the musculoskeletal system and spine, there are many chiropractors who purport treatment of nearly all medical ailments. These chiropractors hold on to age-old beliefs that are steeped in a spiritual mysticism and vitalism.
The invention of chiropractic is attributed to D.D. Palmer. Palmer was originally a magnetic healer who appropriated the osteopathic technique of joint manipulation. He further appropriated the medical term “subluxation” to refer to what he thought were misaligned vertebrae. Positing that these misalignments impinge on nervous tissue which control healing forces within the body, Palmer implicated subluxations as the root cause for all manner of disease. In his book The Science, Art and Philosophy of Chiropractic, he claimed:
D.D. Palmer’s practice of chiropractic may never have gained the following it has today if it weren’t for the mythologizing of a particular extraordinary deed. In 1895 – examining the back of the hearing impaired Harvey Lillard – Palmer claimed to have discovered a bony protrusion. By performing a manual adjustment of the offending vertebrae, Palmer was credited with restoring Lillard’s hearing.
Although the incident is often said to be instrumental to the proliferation of chiropractic, treatment of the deaf is not something found within the scope of modern chiropractic. In fact, no chiropractor has performed the procedure successfully under controlled conditions. The challenge of repeating this chiropractic miracle is likely attributable to the anatomy of hearing (something we now more clearly understand); the auditory nerves reside exclusively within the skull and at no point travel down the spine. To put it bluntly: chiropractic cannot heal the deaf.
As chiropractic first expanded, some practitioners incorporated radical religious and philosophical beliefs. The adoption of religious symbolism and ideology was – in part – a ploy by Palmer to protect chiropractors from prosecution for practicing medicine without a license. Although much of Palmer’s writings were contradictory and far from concise, his philosophy generally describes a Universal Intelligence (God) that manifests as an Innate healing power channeled through the nervous system and spine.
In essence, Palmer’s principles of chiropractic assert that subluxations result in interference between the Innate vitalistic force and the body by compressing the nerves, causing disease. When chiropractors perform adjustments on patients, they claim to be completing the body’s connection with Innate, allowing it to perform its healing ability. It is this practice that led chiropractors to coin the notion of, “connecting man the physical with man the spiritual,” which is often expressed as turning people’s power on.
Of course, no one would believe these things in this modern age would they? Actually, London’s own celebrity chiropractor B.J. Hardick evidently subscribes to a very similar worldview:
While many current practices today developed from mythologies of the past, chiropractic is unique for retaining much of its philosophical and religious heritage. It’s not uncommon today to hear chiropractors reference Innate or subluxations within their practice. Although the term subluxation does have an appropriate medical use, chiropractors have manipulated it to fit their own design. The lack of substantiation for vertebral subluxationdid little to impede the proliferation of chiropractic.
If subluxations are a valid source of concern, we should be able to identify them, illustrate their causal link to disease, and demonstrate that their treatment has a positive effect on specific disease processes and patient symptoms. In 2009, a group of chiropractic researchers examined the evidence relating to subluxations and found “no supportive evidence . . . for the chiropractic subluxation being associated with any disease process or of creating suboptimal health conditions.” Some chiropractors took issue with the findings, but none put forward a substantive critique. Indeed, when suggesting a novel scientific paradigm, the burden of proof rests on those who make extraordinary claims.
In his book Chiropractic Abuse: An Insider’s Lament, chiropractor Preston Long details how the chiropractic profession is plagued by unscientific beliefs that have persisted in spite of their clash with modern scientific and medical knowledge:
“I am a chiropractor. I do not say this with pride. My profession is full of men and women who exaggerate what they can do and provide unnecessary and sometimes dangerous services to their patients. Most chiropractors are not bad people, but far too many embrace cult-like beliefs.”
Today, a contentious rift exists within the chiropractic community. There even exists terminology to demarcate between those clinging to the ideas of the past and those who incorporate novel techniques: straights (often self-described as principled) are those who follow the classical Palmer doctrine whereas mixers are those who incorporate other techniques including modern scientific understanding of disease processes (although mixers sometimes pursue equally suspect health practices). This leaves us with two different chiropractic philosophies. The former (the straights) generally believe that subluxations are the root cause of most disease and that a lifetime of spinal adjustments is essential for maintaining proper health. The latter (the mixers) apply spinal manipulation therapy to relieve musculoskeletal pain and generally work with patients to improve mobility and function.
So if the subluxation is a mythical concept, what benefits do chiropractors offer? A 2011 Cochrane review examined the use of combined chiropractic interventions for what chiropractors are most known for: treatment of lower back pain. While they found evidence that “chiropractic interventions slightly improved pain and disability in the short term and pain in the medium term for acute/subacute” lower back pain, they concluded that “there is currently no evidence that supports or refutes that these interventions provide a clinically meaningful difference for pain or disability in people with [lower-back pain] when compared to other interventions.” Follow up research examining spinal manipulation therapy reached a similar conclusion in 2013.
In addition to lower back pain, there is some evidence indicating that spinal manipulation may aid migraines, as well as neck pain. While the evidence is weak, this may be a result of biomechanical variability among patients, causing some patients to respond well to treatment but not others. After all, many patients swear by chiropractic; while recent Gallup polls illustrated that the American public finds physical therapy generally more effective and safer than chiropractic for neck and back pain, chiropractic care did rank higher than all other interventions. Indeed, many patients are satisfied with their chiropractic care. Despite the mixed evidence, there may be a future for spinal manipulation therapy in treating some pain and disability. If chiropractors can help curtail the opioid crisis as they purport, then their deployment in conservative musculoskeletal care is welcomed.
Unfortunately, a significant impediment to healthcare integration is the division within the chiropractic community. Chiropractic’s historical baggage has led to disparate professional identities, causing criticism from the medical community, particularly among orthopedic surgeons. It’s not hard to see why. Many chiropractors make outlandish and unsubstantiated claims regarding treatment of conditions unrelated to the musculoskeletal system. While evidence-based practitioners generally offer manipulations with the intent of mobilizing joints, those in the straight community claim to precisely adjust misaligned vertebrae and restore them to their proper positions. These claims are dismissed even by chiropractic researchers, yet many practitioners still offer these unscientific services.
A Legacy of Anti-Science
Subluxation-based chiropractic is a treatment in search of a disease. Unlike most medical research which seeks to evaluate novel treatments and diagnostic techniques, chiropractic research is still trying to vindicate an age-old approach to health. This led the American Medical Association to label chiropractic an “Unscientific Cult” as early as 1969. In response, chiropractors sued. Though the AMA lost in an antitrust suit (not by scientific merit), the war continues to this day and chiropractors have still not demonstrated the existence of the subluxation.
In contrast to health practices like physiotherapy or massage, subluxation-based chiropractors are particularly vocal in their opposition to the medical system. A likely explanation – aside from the obvious history – is that physiotherapy, massage, and even modern chiropractic are exclusively complementary to medical practices. Quite distinctly, subluxation-oriented chiropractors often find themselves in competition with the medical system; after all, subluxation-based chiropractors consider their treatment to remedy the cause of most afflictions (despite the lack of evidence). A simple Google search involving the term ‘chiropractic’ and any disease will produce unsavory results. Even chiropractic’s patriarch D.D. Palmer spent time in jail for practicing medicine without a license.
Perhaps the most repugnant philosophical stance that remains pervasive in the chiropractic world is the fervent opposition to vaccination. While scientists and public health experts unanimously recognize vaccination as an effective approach to prevent disease with little risk, the topic remains a contentious issue within the world of chiropractic. D.D. Palmer’s son, B.J. Palmer – the great promoter of chiropractic – is largely responsible.
“The idea of poisoning healthy people with vaccine virus . . . is irrational. People make a great ado if exposed to a contagious disease, but they submit to being inoculated with rotten pus, which, if it takes, is warranted to give them a disease.”
Source: B.J. Palmer’s The Science of Chiropractic: Its Principles & Adjustments
“My parents chose to opt me out of the routine vaccination schedule many years before the world was paying attention to mercury toxicity, Autism, studies, or anything else … My parents wanted me to develop my immune system naturally, without interference.”
Anti-vaccination beliefs aren’t the only risk posed to children by chiropractors. One area in particular where chiropractic has received extensive criticism from the medical community is in the domain of pediatrics. Many chiropractors in Ontario and abroad have made outlandish claims with regards to chiropractic treatment for infants and children. While there are documented consequences from chiropractors working on infants, precise rates of complication are unknown – likely a consequence of poor adverse event documentation and reporting.
“There’s nothing that I love more than seeing a kid jumping up on the table . . . make sure they’re subluxation free and whether it ever elicits a symptomatic change in that child or not, just being able to know that we’ve turned on the power.”
B.J. Hardick is a prominent example of a chiropractor promoting treatments for infants and children. The following images were all scraped from his professional Facebook page:
This slideshow requires JavaScript.
The absurdity of chiropractors treating infants is only eclipsed by what they claim they are treating; many chiropractors advocate for treatment of children with ear infections, asthma, colic, and other non-musculoskeletal conditions. It’s important to note that the vast majority of conditions that chiropractors treat in children are self-limiting – they tend to resolve spontaneously. A prominent example is colic, for which there is no evidence supporting chiropractic treatment.
In Canada, the problem is pervasive enough that the Canadian Pediatric Society released a position paper: “Chiropractic care for children: Controversies and issues”. The original position was posted in 2002 and reaffirmed in 2016. When examining the scientific evidence, they found that there was no evidence for chiropractic to treat any pediatric disorder. Instead, they found that chiropractors put children at risk by spreading misinformation regarding immunization and by attempting to treat acute pediatric conditions that instead need serious medical treatment. These weren’t the only risks identified. The authors noted that “parents should be made aware that there is a lack of substantiated evidence for the theory of subluxated vertebrae as the causality for illness in children, and x-rays taken for this purpose expose the child to unnecessary radiation.” In fact, chiropractors often overuse x-rays. Even for lower back pain, Choosing Wisely Canada recommends against x-rays partly because it has not been shown to improve management of symptoms. Naturally, misuse of X-ray technology has a long history in chiropractic. B.J. Hardick himself claims that it’s dangerous to adjust without x-rays and has showcased x-rays of children in his YouTube videos.
In a further affront (conscious or otherwise) to public health, many chiropractors attribute risk of subluxation to how the baby is delivered (here is a prime example). Not only are they doing a disservice to public health, but they are unnecessarily shaming mothers about their personal choices regarding the birth process.
“The more natural the delivery, the less interference, the fewer interventions medically that are necessary, the less trauma to the skull . . . I had a baby last week where unfortunately based on the way the baby was presented, they had to turn the baby manually inside the mom and then pull the baby out. So the baby’s neck was definitely subluxated.”
“One fact we do know, however, is that the first subluxation usually happens in the birth canal because of the normal trauma associated with vaginal deliveries. Even babies delivered by C-section are subject to birth trauma and vertebral subluxation. This is why it is absolutely critical for parents to bring their babies to their chiropractor as soon after birth as possible. This will ensure that their child’s nervous system is functioning at full capacity, which will provide the framework for a long life of health and vitality.”
In 1991, chiropractors became authorized to use the title ‘doctor’ under the Chiropractic Act. This privilege has been used irresponsibly by chiropractors nation-wide when making public statements on medical concerns unrelated to musculoskeletal issues. When the public is likely to conflate the use of the title ‘doctor’ with ‘medical doctor’, it is irresponsible to apply the title in the context of non-musculoskeletal medical advice; this is especially true when practitioners are disseminating misleading information.
The College of Chiropractors of Ontario is the self-regulating body for chiropractic in Ontario. As authorized in the Chiropractic Act, the chiropractic scope of practice is as follows:
The practice of chiropractic is the assessment of conditions related to the spine, nervous system and joints and the diagnosis, prevention and treatment, primarily by adjustment, of,
(a) dysfunctions or disorders arising from the structures or functions of the spine and the effects of those dysfunctions or disorders on the nervous system; and
(b) dysfunctions or disorders arising from the structures or functions of the joints.
The problem is that the application and enforcement of this scope is open to broad interpretation. If you subscribe to the classical subluxation philosophy and believe that spinal adjustments channel the healing power of Innate through the body, what could possibly be considered outside of a chiropractor’s scope of practice?
How pervasive is the belief among practitioners that chiropractic can effectively treat a wide range of medical conditions unrelated to the spine? Unfortunately, it is not known. No regulatory body surveys and disseminates this information and existing literature on the topic is unreliable at best. A recent survey of Canadian chiropractors indicated that large proportions of chiropractors in clinical practice use entirely unsubstantiated diagnostic and treatment techniques (for example, 22% claimed to prescribe homeopathy – a treatment that isn’t only unproven but implausible).
Ultimately, the regulatory body has not enforced evidence-based practices, resulting in a vast number of chiropractors who sell useless, even dangerous treatments. My article regarding the Byron-based chiropractor who uses a cheap ear thermometer to diagnose subluxations is a prime example of a chiropractor running a successful business in spite of either having no idea what he is doing, or consciously conning his patients. It’s worth repeating: where are the regulators?
Unfortunately, patients seeking responsible chiropractic care must be extra diligent in screening their care provider. My advice would be to take time to examine the chiropractor’s website. Do they make absurd claims regarding non-MSK conditions? Do they treat infants? Do they treat subluxations? Do they offer long-term treatment/payment plans? Do they advertise testimonials regarding conditions outside of the scope of chiropractic? Do they perform x-rays on every patient? If the answer is yes to any of these, you’re very likely dealing with a quack.
“Good chiropractors are essentially physical therapists who specialize in the spine. Spinal manipulation is an effective option for mechanical low back pain, but physical therapists and some doctors also use that treatment. Some chiropractors want to be primary care providers and treat a variety of non-MSK diseases, but they are not trained to do that. Many chiropractors subscribe to outright quackery like applied kinesiology; and only half of them support vaccination. A medical subluxation is a partial dislocation of a joint that is readily visible on x-ray; the “chiropractic subluxation” is a myth and does not show on x-ray. And chiropractic can be dangerous: stroke is a rare but devastating complication of neck manipulations.”
Facebook does not care about your privacy. They aren’t alone; we pay to use all manner of application and platform with our privacy. It’s the price of free. However, I suspect many of us would be more selective with our personal information if we really knew the scope of intrusion. While options are given to users under the guise of Privacy Controls, these are not much more than wool over the eyes. To really understand what’s exposed, you have to think and act like an investigator.
The field of Open Source Intelligence (OSINT) is a passion of mine that focuses on the tools and techniques to uncover information of a target over the internet. Because it’s only peripherally related to the theme of this blog, I’ll take you through the motions using a health-related target who I honed my skills on: chiropractor B.J. Hardick.
I first learned about B.J. through a flyer distributed around town (London, Ontario):
B.J. Hardick Cancer Killers Flyer (Scanned by me in 2016)
The book is a dreadful amalgamation of dangerous and ineffective alt-med practices that goes as far as recommending chiropractic spinal manipulation as cancer treatment. The book was advertised as a sort of manual that recommends dubious techniques used by chiropractor Charles Majors who was diagnosed with multiple myeloma. Although B.J. claimed that Majors cured himself using techniques presented in the book, the tragic irony is that Majors passed away earlier this year. This is a story for another post, however.
So how does this tie in to Facebook privacy? The public presence of alt-med gurus is very different than typical medical professionals. Success is less about providing sound evidence-based care, and more about relentless promotion through social media. In many situations, such social media accounts are identified as professional extensions of practitioners’ clinical practices, which means that sharing silly memes comparing vaccines to events like the holocaust may very well be in the purview of regulatory discipline. So let’s dig in.
B.J. Hardick is evidently tied to three Facebook accounts: his personal page, his professional page, and his clinic’s page. His personal page is obviously out of scope for this investigation and his clinical page is certainly within scope. While his professional page isn’t explicitly linked to his clinical practice, he shares health and medical information and uses the title of Doctor, which is a regulated title in Canada. Hence, this page is in scope.
The simplest approach to investigations on Facebook is Facebook’s own search. It’s actually rather powerful.
Hardick Chiropractic Centre Vaccines – Retrieved December 2017 from: https://www.facebook.com/search/pages/?q=Hardick%20Chiropractic%20Centre%20vaccine
A simple search reveals that the Hardick Chiropractic Centre account has directly disseminated anti-vaccine propaganda that still remains available despite recent warnings to B.J. from the College of Chiropractors of Ontario. Not impressed? Alright, let’s go deeper.
Every Facebook page or account is associated with a numerical ID. Using these IDs, we can make use of Facebook’s graph API, which opens up a vast arsenal of creeping – err – investigating possibilities. Facebook hides these IDs within the source of each page. To view the source (in Chrome), simply right click a page and select “View Source.”
Don’t fret at the incoming wall of code; all we need to do here is search for a single item. If you’re on someone’s personal profile, you want to find the value of profileid. Simply hit Ctrl+F and type in profileid. If, as in this case, you’re not on a personal page but a professional page, you’ll want to find the value of pageid, which appears as follows in this example:
This number is our ticket to the wealth of information we can extract from Facebook. You now have two options. You can learn how Facebook’s Graph API works, or you can use any number of pre-built tools to generate searches for you. Simple, but effective is graph.tips. However, Michael Bazzell’s Intel Techniques has become a household name in the OSINT world due to its comprehensive search tools. Navigate to the Facebook page and you’ll find a form for a Facebook User Number. This is where you place the pageid or profileid value. Click Populate All and you will see a plethora of options. Click Go on any of these and the website will direct you to Facebook with the appropriate search URL.
Examining the pages liked by B.J.’s professional account, we see a frightening trend:
This slideshow requires JavaScript.
Photos posted, liked, and commented on also portray at least a modest disregard for science and public health (even Health Canada has issued an alert regarding mammography):
This slideshow requires JavaScript.
Perhaps most disturbing is that B.J. likes his own posts:
B.J. Hardick Likes His Own Posts. Retrieved Dec. 2017 from: https://www.facebook.com/DrHardick/
What has the world come to?
As our personal and professional lives slowly become entangled in the web of social media, it’s worth taking some time to explore what is revealed about us. I encourage readers to use these tools on their own accounts. Take back your privacy.


























{kind=link}
{kind=link}
{kind=link}
{kind=link}